About Me

Friday, October 30, 2009
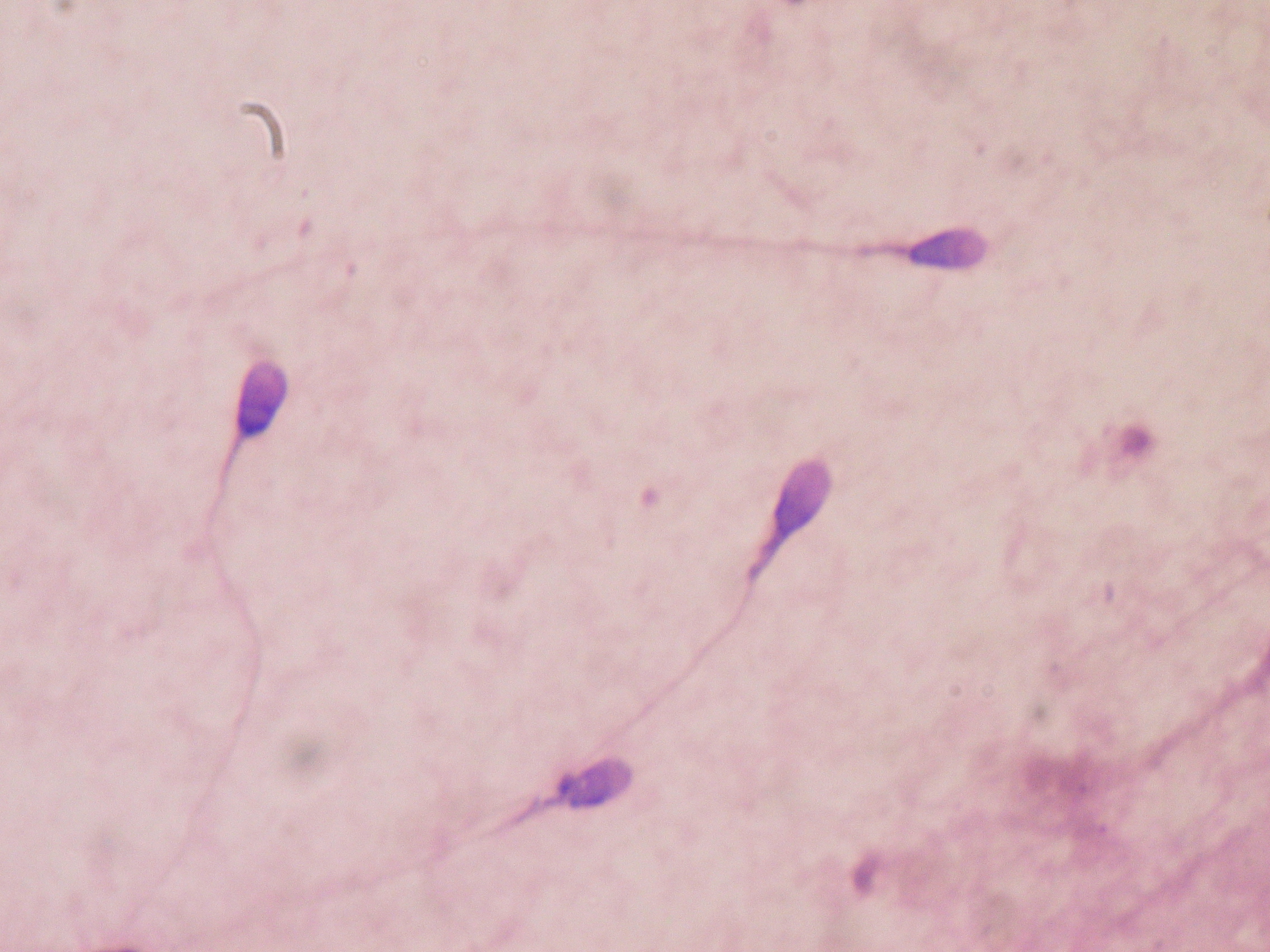
Semen analysis
A semen analysis evaluates certain characteristics of a male's semen and the sperm contained in the semen. It may be done while investigating a couple's infertility or after a vasectomy to verify that the procedure was successful.
Relation to fertility
The characteristics measured by semen analysis are only some of the factors in semen quality. One source states that 30% of men with a normal semen analysis actually have abnormal sperm function.[1] Conversely, men with poor semen analysis results may go on to father children.[2][3]
Collection methods
The most common way to collect a semen sample is through masturbation, directing the sample into a clean cup.[2]
A sample may also be collected during intercourse in a special type of condom known as a collection condom. Collection condoms are made from silicone or polyurethane, as latex is somewhat harmful to sperm.[4] Many men prefer collection condoms to masturbation, and some religions prohibit masturbation entirely. Adherents of religions that prohibit contraception, such as Catholicism, may use collection condoms with holes pricked in them.[5]
A third option for collecting a sample is through coitus interruptus (withdrawal). With this technique, the man removes his penis from his partner near the end of intercourse and ejaculates into a cup.
Finally, if a blockage in the vas deferens is suspected to impede fertility, semen can be taken directly from the epididymis. Such a collection is called per cutaneous epididymal sperm aspiration (PESA). Alternatively, the testicular tissue itself, instead of the sperm produced can be investigated. Then, the collecting method is called TESE.[6]
Tested characteristics
Examples of parameters measured in a semen analysis are: sperm count, motility, morphology, volume, fructose level and pH.
1. Sperm count
Approximate pregnancy rate varies with amount of sperm used in an artificial insemination cycle. Values are for intrauterine insemination, with sperm number in total sperm count, which may be approximately twice the total motile sperm count.
Sperm count, or sperm concentration to avoid mixup, measures the concentration of sperm in a man's ejaculate, distinguished from total sperm count, which is the sperm count multiplied with volume.[7] Anything over 20 million sperm per milliliter is considered normal.[1][2] Anything less is considered oligospermia. A vasectomy is considered successful if the sample is azoospermic. Some define success with rare non-motile sperm are observed (fewer than 100,000 per millilitre).[8] Others advocate obtaining a second semen analysis to verify the counts are not increasing (as can happen with re-canalization) and others still may perform a repeat vasectomy for this situation.
The average sperm count today is around 60 million per milliliter in the Western world, having decreased by 1-2% per year from a substantially higher number decades ago.[9]
2. Motility
The motility of the sperm is evaluated. WebMD defines normal motility as 60% of observed sperm, or at least 8 million per millilitre, showing good forward movement.[2] The World Health Organization has a similar value of 50% and this must be measured within 60 minutes of collection. A man can have a total number of sperm far over the limit of 20 million sperm cells per milliliter, but still have bad quality because too few of them are motile. However, if the sperm count is very high, then a motility of less than 60% might not matter, because the fraction might still be more than 8 million per millilitre. The other way around, a man can have a sperm count far less than 20 million sperm cells per millilitre and still have good motility, if more than 60% of those observed sperm cells show good forward movement.
A more specified measure is motility grade, where the motility of sperm are divided into four different grades:[10]
- Grade 4: Sperm with progressive motility. These are the strongest and swim fast in a straight line. Sometimes it is also denoted motility a.
- Grade 3: (non-linear motility): These also move forward but tend to travel in a curved or crooked motion. Sometimes also denoted motility b.
- Grade 2: These have non-progressive motility because they do not move forward despite the fact that they move their tails.
- Grade 1: These are immotile and fail to move at all.
3. Morphology
The morphology of the sperm is also evaluated. With WHO criteria as described in the old manual of 1989, a sample is normal if 30% or more of the observed sperm have normal morphology.[1] If morphology is evaluated using the Tygerberg strict criteria developed by Dr. Roelof Menkveld, Tygerberg Hospital, South Africa, and disseminated by Dr. Thinus Kruger from the same hospital,[11] a sample is normal if 14% or more of the observed sperm have normal morphology.[1]. The Tygerberg strict criteria for morpology assessment are recommended in the most recent WHO manual on semen analysis (WHO 1999). According to the above references, morphology was developed as a predictor of success in fertilizing oocytes during invitro fertilization.
4. Volume
The volume of the sample is measured. WebMD advises that volumes between 1.0 mL and 6.5 mL are normal;[2] WHO criteria specify that any volume greater than 2.0 mL is normal. Low volume may indicate partial or complete blockage of the seminal vesicles, or that the man was born without seminal vesicles.[1] In clinical practice, a volume of less than 2 mL in the setting of infertility and absent sperm should prompt an evaluation for obstructive azoospermia. A caveat to this is be sure it has been at least 48 hours since the last ejaculation to time of sample collection.
5. Fructose level
The level of fructose in the semen is measured. WebMD lists normal as at least 3 mg/mL.[2] WHO specifies a normal level of 13 μmol per sample. Absence of fructose may indicate a problem with the seminal vesicles.[1]
6. pH
The pH of the sample is measured. WebMD lists a normal range of 7.1-8.0;[2] WHO criteria specify normal as 7.2-7.8.[1] Acidic ejaculate (lower pH value) may indicate one or both of the seminal vesicles are blocked. A basic ejaculate (higher pH value) may indicate an infection.[1] A pH value outside of the normal range is harmful to sperm.[2]
7. Liquefaction
The liquefaction is the process when the gel formed by proteins from the seminal vesicles is broken up and the semen becomes more liquid. It normally takes less than 20 minutes for the sample to change from a thick gel into a liquid. An abnormally long liquefaction (more than 30 minutes at 37 24°C) time may indicate an infection.
8. MOT
MOT is a measure of how many million sperm cells per ml are highly motile[12], that is, approximately of grade 4, or sometimes also taking grade 3 into account. Thus, it is a combination of sperm count and motility.
With a straw volume of 0.5 milliliter per straw, the general guideline is that, for intracervical insemination (ICI), straws making a total of MOT40 is recommended. This is equal to 8 straws with MOT5, or 2 straws of MOT20. For intrauterine insemination (IUI), straws making a total of MOT10 is regarded sufficient.[13] In WHO terms, it is thus recommended to use approximately 20 million grade 3+4 sperm in ICI, and 5 million ones in IUI.
Total motile spermatozoa
Total motile spermatozoa (TMS)[14] or total motile sperm count (TMSC)[15] is a combination of sperm count, motility and volume, measuring how many million sperm cells in an entire ejaculate are motile.
Use of approximately 20 million grade 3+4 sperm in ICI, and 5 million ones in IUI may be an approximate recommendation.
9. Others
The sample is tested for white blood cells. A high level of white blood cells (over 1 million per milliliter) may indicate an infection.[1]
Abnormalities
- Aspermia: absence of semen
- Azoospermia: absence of sperm
- Oligospermia: low number of sperm
- Asthenozoospermia: poor sperm motility
- Teratozoospermia: sperm carry more morphological defects than usual
Factors that influence results
Compared to samples obtained from masturbation, semen samples from collection condoms have higher total sperm counts, sperm motility, and percentage of sperm with normal morphology. For this reason, they are believed to give more accurate results when used for semen analysis.[4]
How long the man has abstained prior to providing the sample for analysis affects the results. Longer periods of abstinence correlate with poorer results - one study found that men with repeated normal results produced abnormal samples if they abstained for more than 10 days. It is recommended not to abstain for more than one or two days before providing the semen sample for analysis.[16]
If the results from a man's first sample are subfertile, they must be verified with at least two more analyses. At least 2 to 4 weeks must be allowed between each analysis.[17] Results for a single man may have a large amount of natural variation over time, meaning a single sample may not be representative of a man's average semen characteristics.[18] In addition, sperm physiologist Joanna Ellington believes that the stress of producing an ejaculate sample for examination, often in an unfamiliar setting and without any lubrication (most lubricants are somewhat harmful to sperm), may explain why men's first samples often show poor results while later samples show normal results.[3]
A man may prefer to produce his sample at home rather than at the clinic. The site of semen collection does not affect the results of a semen analysis.[19]
Measurement methods
Volume can be determined by measuring the weight of the sample container, knowing the mass of the empty container. Sperm count and morphology can be calculated by microscopy. Sperm count can also be estimated by kits that measure the amount of a sperm-associated protein, and are suitable for home use. [20]
Computer Assisted Semen Analysis (CASA) is a catch-all phrase for automatic or semi-automatic semen analysis techniques. Most systems are based on image analysis, but alternative methods exist such as tracking cell movement on a digitizing tablet.[21][22] Computer-assisted techniques are most-often used for the assessment of sperm concentration and mobility characteristics, such as velocity and linear velocity. Although many systems can give very accurate information about motility patterns of motile sperm, immotile sperm cannot accurately be distinguished from other cells, particles or debris without addition of staining. The first CASA systems in general cannot give reliable results for sperm concentration and proportions of sperm with different grades of motility, at least not in semen samples, where there are many other particles, cells and debris. Even when it comes to motility, most systems cannot give reliable results when the concentration of motile sperm leads to significant "crossed paths" - due to difficulties to decide if there were two sperm crossing each others way, or if there were for instance four sperm moving close to each other. Nowadays, there are CASA systems, based on image analysis and using new techniques, with near perfect results, and doing full analysis in a few seconds.
CASA Systems
SQA-V - The SQA-V, also known as the 'Sperm Quality Analyzer or Spermalite, is a high performance sperm analysis instrument used to test male fertility. It combines electro-optics, computer algorithms and video microscopy to provide a precise and accurate 75 second automated semen analysis. This device is manufactured by Medical Electronic Systems [23], who specializes in rapid, automated semen analysis. The main reason the SQA-V is a growing instrument among the semen analysis community is due to the speed, accuracy, and precision to run a semen sample. In addition, the SQA-V semen analysis eliminates inter-operator variables from the manual method, and still provides 16 clinical parameters including: Sperm Concentration, Rapid Progressive motility, Slow Progressive motility, Non-progressive motility, Immotility, %Normal Morphology, and more.
A study was conducted by the world renowned Cleveland Clinic comparing the SQA-V to the Manual method and the CASA device, presenting results favoring the SQA-V. [24]
ISAS - Integrated Semen Analysis System is a CASA system based on image analysis from the company Projects i Serveis R+D S.L., also known as PROISER. PROISER was founded on 2004 by a team of CASA developers (SCA 96, SCA 98 and SCA 2002) with more than 15 years in experience of seminal analysis by computer image analysis. ISAS can be considered as the most complete and easiest-to-use system in market which, furthermore, works in different hardware and operating-system conditions, in order to adapt as much as possible to the needs of our users. Current computers and AAVT technology allows a very good matching of spermatozoon, thanks to the tail and morphology analysis made at the same time as motility analysis. Only motility and concentration analysis give to the customers more tan 17 sperm parameters, but also ISAS analyzes automatically stained morphometry, giving 15 parameters and DNA fragmentation analysis. ISAS has been developed to be used in several species, from classical species like human, boar or bull to new research species like cod or some small rodents. There are a lot of publications and works in progress with ISAS like [25]. A list of last publications with this CASA system can be found on publications with ISAS
Sperm Class Analyzer - The Sperm Class Analyzer, also known as 'SCA' from the company Microptic S.L., provides fast, accurate and objectively repeatable results. This would be impossible to attain using traditional (subjective) methods. This CASA system has the following modules: SCA Motility & Concentration: The system provides immediately and objectively detailed results of motility and concentration in a complete report. SCA Morphology: Following a manual or automatic image capture, a precise morphological and morphometric analysis of each spermatozoid is provided in real time. SCA DNA Fragmentation: Analysis of halo formation of the samples prepared for study of the DNA fragmentation provides detailed numerical data for each of the cells. SCA Vitality: Automatically analyze the vitality of a sperm sample. All this modules can be used with a motorized stage or link the database with any hospital system.
IVOS Sperm Analyzer - The Integrated Visual Optical System (IVOS) was developed by Hamilton Thorne, the leading manufacturer of CASA systems since 1986. The IVOS is found in hospitals, universities, IVF clinics, pharmaceutical companies, contract labs, reproductive toxicology labs, veterinary clinics and animal breeding facilities around the world. The standard IVOS software may be used to analyze sperm of multiple species, with a specific program geared toward analysis of rat sperm. The IVOS is unique in that it is the only CASA system that integrates the optical system within the unit, so that an external microscope is not needed. The light source of the IVOS produces stroboscopic illumination to provide blur free sperm images. This stroboscopic light source is especially beneficial when utilizing the IDENT fluorescent option on the IVOS as it allows the analysis of motile sperm under fluorescent illumination without adverse affect on sperm motility or velocity (this is not possible with continuous light fluorescent microscopes). Analysis using the IVOS IDENT provides highest accuracy of sperm counts in samples with a high degree of detritus, such as occurs in egg yolk extended samples or naturally in some species, such as rabbits. Samples are placed on a computer-controlled, heated stage which maintains samples at the proper analysis temperature and automatically moves to selected fields for analysis. A field of sperm are analyzed in just 0.5 second with a level of accuracy and repeatability unobtainable by visual assessment. Results calculated include count, concentration, motility, progressive motility, curvilinear velocity (VCL), straight line velocity (VSL), average path velocity (VAP), linearity (LIN), straightness (STR), amplitude of lateral head displacement (ALH) and beat cross frequency (BCF). Custom software packages are available, such as Animal Breeder, Equine Breeder and Animal Motility, which provide additional features specific to the target industries. In addition, the TOX IVOS is a complete system configured specifically for the inticacies of rat sperm analysis. Two automated morphology options, Dimesnisons Strict Morphology (developed and validated by Dr. Thinus Kruger) and Metrix user defined morphology are available. Another fluorescent option is VIADENT, which permits the analysis of motility and viability on the same live sample.
"Our results suggest that the VIADENT option of the IVOS system is capable of a rapid, accurate and objective evaluation of both viability and motility parameters using large numbers of spermatozoa. Application of this technique in the industry may prove useful in the clinical assessment of fertilizing potential of equine spermatozoa." [26]
CEROS Sperm Analyzer - Also from Hamilton Thorne and built upon the same analysis algorithms and software interface as the IVOS, the CEROS offers the same level of accuracy and reliability for sperm analysis. The CEROS uses an external negative phase contrast microscope for image visulaization and analysis. The system comes complete with motility analysis software, microscope, camera, computer and monitor. The CEROS is also compatible with both the Dimensions and Metrix morphology options and can be used for to analyze sperm from all species except rat. Both systems offer 4 levels of quality control as well as high-level security and audit trail for data inetgrity. A searacble list of publications featuring the Hamilton Thorne IVOS and CEROS CASA systems is found on Connotea.
References
- "Understanding Semen Analysis". Stonybrook, State University of New York. 1999. http://www.uhmc.sunysb.edu/urology/male_infertility/SEMEN_ANALYSIS.html. Retrieved 2007-08-05.
- Essig, Maria G.; Edited by Susan Van Houten and Tracy Landauer, Reviewed by Martin Gabica and Avery L. Seifert (2007-02-20). "Semen Analysis". Healthwise. WebMD. http://www.webmd.com/infertility-and-reproduction/guide/semen-analysis?page=1. Retrieved 2007-08-05.
- Ellington, Joanna (2004). "Understanding a Sperm Analysis". INGfertility. http://www.preseed.com/FAQs/FAQ4.php. Retrieved 2008-06-28.
- Dr. Joanna Ellington (January 2005). Use of a Specialized Condom to Collect Sperm Samples for Fertility Procedures. INGfertility. http://www.preseed.com/FAQs/FAQ4.php#Using_a_Sperm_Collection_Condom. Retrieved 2008-06-28.
- Kippley, John; Sheila Kippley (1996). The Art of Natural Family Planning (4th addition ed.). Cincinnati, OH: The Couple to Couple League. pp. pp.306–307. ISBN 0-926412-13-2.
- Fertility Center, Stockholm (translated from Swedish)
- sharedjourney.com - Male Infertility Testing
- Rajmil O, Fernández M, Rojas-Cruz C, Sevilla C, Musquera M, Ruiz-Castañe E (2007). "Azoospermia should not be given as the result of vasectomy" (in Spanish; Castilian). Arch. Esp. Urol. 60 (1): 55–8. PMID 17408173.
Dhar NB, Bhatt A, Jones JS (2006). "Determining the success of vasectomy". BJU Int. 97 (4): 773–6. doi:10.1111/j.1464-410X.2006.06107.x. PMID 16536771. - The sperm count has been decreasing steadily for many years in Western industrialized countries: Is there an endocrine basis for this decrease? The Internet Journal of Urology TM. ISSN: 1528-8390
- Shared Journey: Semen Analysis
- "Semen analysis morphology". IVF 1. 2005-10-27. http://www.ivf1.com/Semen-analysis-morphology/. Retrieved 2007-08-05.
- Cryos FAQs - What does MOT mean?
- Cryos FAQs - What is the recommended quantity and quality by ordering of donor semen?
- Merviel P, Heraud MH, Grenier N, Lourdel E, Sanguinet P, Copin H (November 2008). "Predictive factors for pregnancy after intrauterine insemination (IUI): An analysis of 1038 cycles and a review of the literature". Fertil. Steril.. doi:10.1016/j.fertnstert.2008.09.058. PMID 18996517.
- Pasqualotto EB, Daitch JA, Hendin BN, et al. (October 1999). "Relationship of total motile sperm count and percentage motile sperm to successful pregnancy rates following intrauterine insemination". J. Assist. Reprod. Genet. 16 (9): 476–82. doi:10.1023/A:1020598916080. PMID 10530401. http://www.kluweronline.com/art.pdf?issn=1058-0468&volume=16&page=476.
- Ellington, Joanna (2005). "How Long to Abstain for a Sperm Test/Analysis". INGfertility. http://preseed.com/FAQs/FAQ1.php#How_Long_to_Abstain_for_a_Sperm_Test/Analysis__. Retrieved 2008-06-28. , which cites:
- Levitas E, Lunenfeld E, Weiss N, et al. (June 2005). "Relationship between the duration of sexual abstinence and semen quality: analysis of 9,489 semen samples". Fertil. Steril. 83 (6): 1680–6. doi:10.1016/j.fertnstert.2004.12.045. PMID 15950636.
- Jurema MW, Vieira AD, Bankowski B, et al. (September 2005). "Effect of ejaculatory abstinence period on the pregnancy rate after intrauterine insemination". Fertil. Steril. 84 (3): 678–81. doi:10.1016/j.fertnstert.2005.03.044. PMID 16169402.
- Weschler, Toni (2002). Taking Charge of Your Fertility (Revised ed.). New York: HarperCollins. pp. p.189. ISBN 0-06-093764-5.
- "Adequate Analysis Frequency". Kokopelli Technologies. 2007. http://www.fertilityformen.com/info_why.php#frequency. Retrieved 2007-08-11.
- Shetty Licht R, Handel L, Sigman M (2007). "Site of semen collection and its effect on semen analysis parameters". Fertil Steril. 89: 395. doi:10.1016/j.fertnstert.2007.02.033. PMID 17482174.
- dailyprogress.com > Charlottesville company sends out its home male sterility tests By Brian McNeill. Published: May 14, 2009
- Mortimer ST (01 Jul 2000). "CASA--practical aspects". J. Androl. 21 (4): 515–24. PMID 10901437. http://www.andrologyjournal.org/cgi/reprint/21/4/515. Retrieved 2007-08-05.
- Hinting A, Schoonjans F, Comhaire F (1988). "Validation of a single-step procedure for the objective assessment of sperm motility characteristics". Int. J. Androl. 11 (4): 277–87. doi:10.1111/j.1365-2605.1988.tb01001.x. PMID 3170018.
- http://mes-ltd.com/overview.asp
- Agarwal A, Sharma R (2007). "Automation is the key to standardized semen analysis using the automated SQA-V sperm quality analyzer". Fertility and Sterility 87 (No. 1): 156. doi:10.1016/j.fertnstert.2006.05.083. http://www.clevelandclinic.org/ReproductiveResearchCenter/docs/agradoc230.pdf.
- L. Ramió, M.M. Rivera, A. Ramírez, I.I. Concha, A. Peña, T. Rigau and J.E. Rodríguez-Gil (2008). "Dynamics of motile-sperm subpopulation structure in boar ejaculates subjected to in vitro capacitation and further in vitro acrosome reaction". Theriogenology 69 (No. 4): 501. doi:10.1016/j.theriogenology.2007.10.021. http://www.sciencedirect.com/science?_ob=ArticleURL&_udi=B6TCM-4RCNPPD-1&_user=10&_coverDate=03%2F01%2F2008&_rdoc=15&_fmt=summary&_orig=browse&_srch=doc-info(%23toc%235174%232008%23999309995%23679613%23FLA%23display%23Volume)&_cdi=5174&_sort=d&_docanchor=&_ct=17&_acct=C000050221&_version=1&_urlVersion=0&_userid=10&md5=9926ba71bee609b30a7c56f73857f511.
- Wessel MT, Althouse GC. Validation of an objective approach for simultaneous assessment of viability and motility of fresh and cooled equine spermatozoa. Proceedings of the International Symposium on Equine Reproduction, Animal Reproduction Science 94 (2006) 21-22
Visitor

SLIDE PRESENTATION



Facebook Badge
Copyright © 2009 Complicated Girl. All Rights Reserved.
1 comments:
Hi,thank you for taking the time to explain and the information given are useful.
ivf hospitals in chennai | fertility treatment in chennai
Post a Comment